
WHAT IS CYSTOSCOPY?
This procedure is used to examine your bladder. Your doctor will insert a cystoscope, which is a thin tube with a camera and light on the end, through your urethra (which is the tube that collects urine from your bladder to the outside of your body) and into the bladder. Small surgical instruments can also be passed down the cystoscope to treat some bladder problems at the same time.
There are 2 types of cystoscopy
Flexible cystoscopy: a thin (about the width of a pencil), bendy cystoscope is used, and you stay awake while it’s carried out.
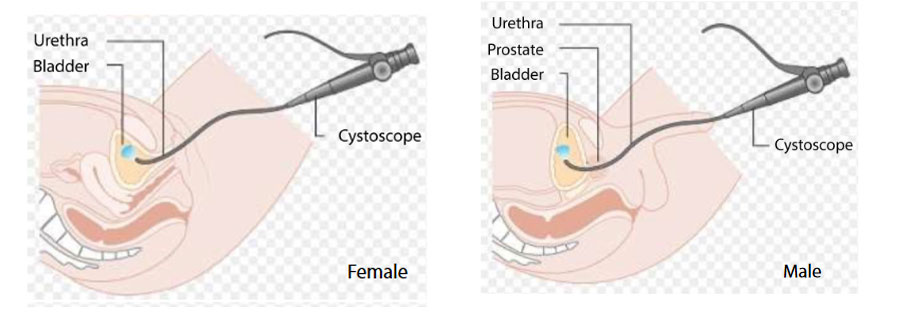
Cystoscopy with a flexible cystoscope
Rigid cystoscopy: a slightly wider cystoscope that does not bend is used, and you may either be put to sleep or the lower half of your body is numbed during the procedure.
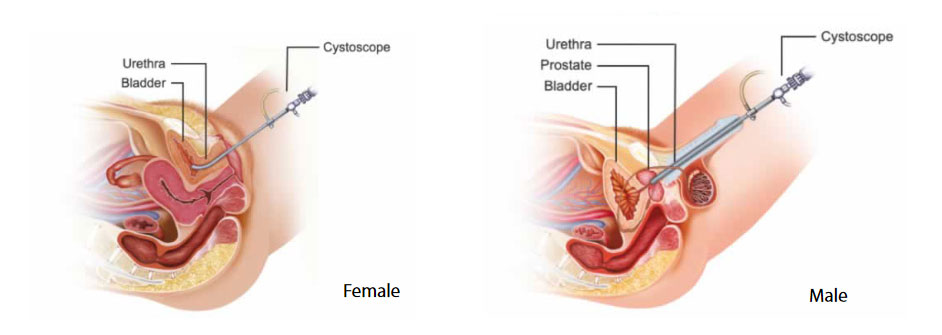
Cystoscopy with a rigid cystoscope
The doctor can look directly down the cystoscope and also images can be displayed on a computer screen or monitor. Both types of cystoscope have side channels where various thin devices can pass down. For example, the doctor may take a small sample (biopsy) from the lining of the bladder by using a thin ‘grabbing’ instrument which is passed down a side channel.
A flexible cystoscope is the type most commonly used. As it is flexible, it usually passes easily along the curves of the urethra. The flexible tip can also be moved easily so a doctor can look at all the inside lining of the bladder. However, a rigid cystoscope allows a greater variety of devices to pass down side channels, which may be needed for various procedures. Large biopsies or removal of tumours, called transurethral resection of bladder tumour (TURBT), are usually performed using a rigid cystoscope.
WHY IS CYSTOSCOPY DONE?
To help with diagnosis
A cystoscopy may be done to help to find the cause of symptoms such as:
- Frequent urinary tract infections;
- Blood in your urine (haematuria);
- Urinary incontinence;
- Unusual cells found in a urine sample;
- Persistent pain when you pass urine;
- Difficulty in passing urine – which may be due to prostate enlargement or a narrowing (stricture) of the urethra.
Cystoscopy may also be done to monitor progress of conditions. For example, some people have a routine cystoscopy every now and then after treatment for a bladder tumour. This helps to detect any early recurrence which can be treated before it spreads further.
To treat certain conditions, or to do certain procedures
By using various instruments which are passed down the side channels a doctor can:
- Remove a stone from the bladder. If a stone is lodged higher – in a ureter – the doctor may extend the cystoscope up into a ureter. The ureters are tubes that drain urine from the kidneys to the bladder;
- Obtain a urine sample from each of the ureters. This helps to check for infection or tumour which involves only one kidney;
- Remove small lumps (polyps) or tumours from the lining of the bladder;
- Insert a small tube (stent) into a narrowed ureter. This helps the flow of urine if there is a narrowing;
- Inject medicine into the bladder;
- Perform a special X-ray of the ureters and kidneys. A doctor can inject a dye into the ureters up towards the kidney. This shows up on X-ray images and helps to show problems of the kidney or ureter;
- Remove the prostate (by using a special type of cystoscope which “chips” away at the prostate gland bit by bit).
WHAT HAPPENS DURING A FLEXIBLE CYSTOSCOPY?
Cystoscopy is usually done as an outpatient or day case. This means you can go home on the same day. Flexible cystoscopy is usually done whilst you are awake. Some people are given a sedative to help them to relax.
You need to wear a hospital gown and lie on your back on a couch. The opening to your urethra (at the end of the penis, or the outside of the vagina) and the nearby skin will be cleaned. Some jelly is then squirted into the opening of the urethra. The jelly usually contains a local anaesthetic to numb the lining of the urethra. This helps the cystoscope to pass into the urethra with as little discomfort as possible.
The doctor will then gently push the cystoscope up into the bladder. The doctor will look carefully at the lining of the urethra and bladder. Sterile water is passed down a side channel in the cystoscope to fill your bladder slowly. This makes it easier for the doctor to see the lining of the bladder. As your bladder fills you will feel the urge to pass urine, which may be uncomfortable.
A flexible cystoscopy takes about 5-10 minutes if it is just to look inside the bladder. It may last longer if the doctor does a procedure – for example, taking a sample (biopsy) from the lining of the bladder. The cystoscope is then gently pulled out. Your doctor may tell you what they saw inside your bladder straight after the test. If you had a biopsy taken, the sample is sent away to be tested and examined under a microscope. It can take several days for the biopsy report to come back to your doctor.
WHAT HAPPENS DURING A RIGID CYSTOSCOPY?
The procedure is done in the operating theatre. You will be given instructions to follow before your appointment. This will include advice with regards to eating, drinking, and what to do about any medications you may be taking.
You will usually need to stop eating and drinking for a few hours before a rigid cystoscopy. You will also need to arrange for someone to give you a lift home, as you will not be able to drive for 24 hours.
You will either be put to sleep for the procedure or the lower half of your body will be numbed (spinal anaesthetic) during the procedure.
The procedure can last up to 30 minutes.
When the procedure is finished, you will be taken to a room or ward to recover from the anaesthetic.
A thin tube called a catheter may have been inserted into your bladder to help you urinate. This will be removed before you go home.
WHAT ARE THE POSSIBLE COMPLICATIONS?
Most cystoscopies are done without any problem. For the following 24 hours you may experience a mild burning feeling when passing urine, and feel the need to urinate more often than usual. Also, your urine may look pink due to mild bleeding, particularly if a biopsy was taken.
Complications include:
- Urinary tract infections: these are the most common complications of a cystoscopy. These are infections of the bladder, kidneys, or small tubes connected to them;
- Being unable to empty your bladder: you will normally be asked to empty your bladder before leaving hospital to make sure you are able to, but sometimes it can become difficult to urinate after going home. This can be a sign that your urethra or your prostate (a small gland found in men) is swollen;
- Bladder damage, that causes important bleeding.
After you have had a cystoscopy, tell your doctor if:
- Pain or bleeding is severe;
- Any pain or bleeding lasts longer than 2 days;
- You develop symptoms of infection, such as a fever, or pain in the lower back or side;
- You cannot empty your bladder;
- Your urine smells bad.
FOLLOW-UP
Any biopsies taken during cystoscopy will be examined under a microscope. These biopsy results can take up to 2 weeks for completion.
During the follow-up appointment, your doctor will explain the findings, if any, to you and whether you need further treatment and follow-up.


