
Table of contents
WHAT IS PREMATURE RUPTURE OF MEMBRANES?
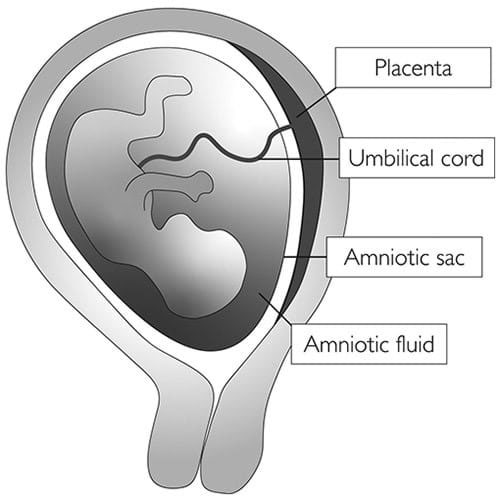
Your baby is surrounded by amniotic fluid or “waters” contained within a membrane bag (the amniotic sac) inside your uterus. It protects and cushions the baby.
Usually, the membranes rupture (waters break) during labour, either spontaneously or by being broken by a midwife or doctor.
Premature rupture of membranes (PROM) is a rupture (breaking open) of the membranes (amniotic sac) before labour begins. If PROM occurs before 37 weeks of pregnancy, it is called preterm premature rupture of membranes (PPROM).
PROM and PPROM occur in up to 3 out of every 100 (3%) pregnant women.
When your waters break early, the sterile sack surrounding your baby is broken. This leaves both you and your baby vulnerable to infection, also you have a higher chance of giving birth prematurely.
WHY DO MEMBRANES RUPTURE BEFORE LABOUR?
Rupture of the membranes near the end of pregnancy (term) may be caused by a natural weakening of the membranes. However, it is often related to an infection in the uterus, due to bacteria from the vagina which crossed intact amniotic membranes.
Other factors that may be linked to PROM and PPROM include the following:
- Cigarette smoking during pregnancy
- Sexually transmitted infections, such as chlamydia and gonorrhoea
- Previous preterm birth
- Vaginal bleeding
HOW WILL I KNOW IF MY WATERS HAVE BROKEN?
You may notice a ‘gush’ of fluid or you may feel damp. The amount of fluid you lose may vary from a trickle to a gush.
WHAT SHOULD I DO?
If you think that you are leaking fluid from the vagina, wear a pad not a tampon and note the colour and amount of the fluid. You should go to the hospital for a check-up straight away.
HOW IS PROM/PPROM DIAGNOSED?
- Membranes rupture is best diagnosed by a vaginal examination. Your doctor will use a sterile speculum(an instrument used to separate the walls of the vagina) to look at your cervix and see whether the leaking fluid is amniotic fluid.
- A swab test of the fluid may help to decide whether your waters have broken, if it is still unclear after the speculum examination.
- An ultrasound scan to estimate the amount of fluid around your baby is sometimes helpful.
WHAT HAPPENS NEXT?
If your waters have broken, you will usually be advised to stay in hospital for a few days, although in some situations this may be for longer.
- You and your baby will be closely monitored for signs of infection.
- This will include having your temperature, blood pressure and pulse taken regularly, together with vagina swab, blood and urine tests to check for infection (results take 3 to 5 days to be available).
- Your baby’s heart rate will also be monitored regularly. You may be advised to have a period of continuous monitoring for at least 20 minutes using a CTG monitor, depending on your risk factors.
If your waters have not broken, you should be able to go home.
If only a very small amount of amniotic fluid is leaking, it is not always easy to see on examination and it can be difficult to confirm whether your waters have broken. If you continue to leak fluid at home, you should return to the hospital for a further check-up.
WHAT ARE THE RISKS OF PROM/PPROM FOR YOU AND YOUR BABY?
Infection
- The membranes form a protective barrier around the baby, and after these have broken, there is a risk of infection getting into your uterus (chorioamnionitis).
- The risk of infection increases as the time between rupture of membranes and birth increases.
- If you have an infection, this can cause you to go into labour early or cause you or your baby to develop sepsis.
- The symptoms of infection include a raised temperature, an unusual vaginal discharge with an unpleasant smell, a fast pulse rate and pain in your lower abdomen. Your baby’s heart rate may also be faster than normal.
- If there are signs that you have an infection, your baby may need to be born straight away to try to prevent both you and your baby becoming more unwell.
Early onset neonatal sepsis (EONS)
- EONS is a blood infection that occurs within the first days of life.
- The baby gets the infection from the mother before or during delivery.
- Risk factors for EONS include maternal chorioamnionitis, maternal colonisation with group B streptococcus, preterm birth and prolonged rupture of membranes (more than 24 hours before delivery).
- Babies born from mothers with PROM/PPROM must be screened for EONS.
- This screening includes blood tests (blood cell count, measurement of C-reactive protein or CRP0 and may include gastric fluid culture.
- If EONS is suspected your baby will be started on antibiotics
- A paediatrician will meet you to explain all details about the management of this condition
Preterm birth
- About 50% of women with PPROM will go into labour within the first week after their waters break. The further along you are in your pregnancy the more likely you are to go into labour within 1 week of your waters breaking.
- Babies born prematurely have an increased risk of health problems, particularly with breathing, feeding and infection, and may need admission to a neonatal unit. The earlier your baby is born, the more likely that this will be the case.
Other complications
- Cord prolapse, when the umbilical cord falls through your cervix into the vagina: this is an emergency complication and can be life-threatening for your baby, but it is uncommon.
- Pulmonary hypoplasia, when your baby’s lungs fail to develop normally because of a lack of fluid around them: this is more common if your waters break very early on in pregnancy (less than 24 weeks) when your baby’s lungs are still developing.
- Placental abruption, when your placenta separates prematurely from your uterus: this can cause heavy bleeding and can be dangerous for both you and your baby.
- If you experience PPROM, sometimes your baby may not survive. The risk of this happening is greater if your waters break very early, if the baby is born very prematurely or, in some cases, following infection or cord prolapse.
ARE THERE ANY TREATMENTS FOR PPROM?
It is not possible to replace the fluid or repair the hole in the membranes around your baby. You may carry on leaking fluid for the rest of your pregnancy as amniotic fluid continues to be made.
If you are 34 weeks or earlier, you will likely be admitted to the hospital. Treatments could include:
- A course of antibiotics to reduce the risk of an infection getting into the uterus and affecting both you and your baby; antibiotics can also help to delay you going into labour;
- Intravenous antibiotics (if you are in preterm labour) to reduce the risk of EOMS due to group B Streptococcus infection;
- A course of steroid injections (corticosteroids) to help your baby’s lungs mature. and to reduce the chance of problems caused by being born preterm;
- Magnesium sulfate, a medication that may be offered to you if your baby is at risk of being born very prematurely; this can reduce the risk of developing cerebral palsy.
If you are between 34 and 37 weeks, depending on the risk of infection from your symptoms and the results of blood tests and others investigations, your doctor will discuss with you about waiting a little bit more to prolong the pregnancy or inducing labour.
If you are at 37 weeks or later, and you don’t go into labour on your own, your doctor will advise inducing labour as soon as you are admitted to hospital.


